Peripheral Artery Disease: Review
Peripheral arterial disease (PAD) is primarily driven by atherosclerosis related to hypertension, diabetes mellitus, hyperlipidemia, and smoking, with microvascular and endothelial dysfunction exacerbating disease progression and complications.
Duplex ultrasound (DUS) is recommended as the first-line, non-invasive imaging modality for PAD diagnosis and surveillance, offering high sensitivity and specificity in most arterial segments while avoiding contrast or radiation exposure, particularly beneficial for patients with renal impairment.
Optimal medical management for PAD includes aggressive risk factor modification (smoking cessation, statin therapy regardless of baseline LDL, antihypertensive therapy, antithrombotic agents—preferably single antiplatelet, and glycemic control in diabetes), with strong evidence supporting supervised exercise therapy for symptomatic relief in claudication.
Endovascular interventions, such as balloon angioplasty (including drug-coated and lithotripsy balloons) and stent placement (preferably nitinol or covered stents for specific lesions), are generally preferred over surgical revascularization for aortoiliac and femoropopliteal disease due to lower morbidity, comparable limb salvage, and improved quality of life outcomes.
Surgical bypass remains the gold standard for complete femoropopliteal occlusions and long or complex lesions, but is associated with higher perioperative morbidity and mortality, making endovascular-first strategy preferable in most other anatomical locations or high-risk patients.
In endovascular therapy, advancements such as 2D fusion imaging and retrograde re-entry catheters have significantly reduced radiation and contrast loads while increasing technical success rates, particularly for chronic total occlusions and challenging anatomy.The choice of revascularization strategy must be individualized based on anatomic lesion (TASC II classification), patient comorbidities and surgical risk, with endovascular-first approaches supported for most lesions except for certain complex infrapopliteal or common femoral artery diseases where open surgery or endarterectomy may yield superior long-term patency.
earn CME at app.embllm.com
This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Scimple Education, LLC, and EMBLLM, LLC. Scimple Education, LLC is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Scimple Education, LLC designates this Enduring Material for a maximum of 24.0 AMA PRA Category 1 Credits™ for physicians. Physicians should claim only the credit commensurate with the extent of their participation in this activity.
Care of Avalanche Patients
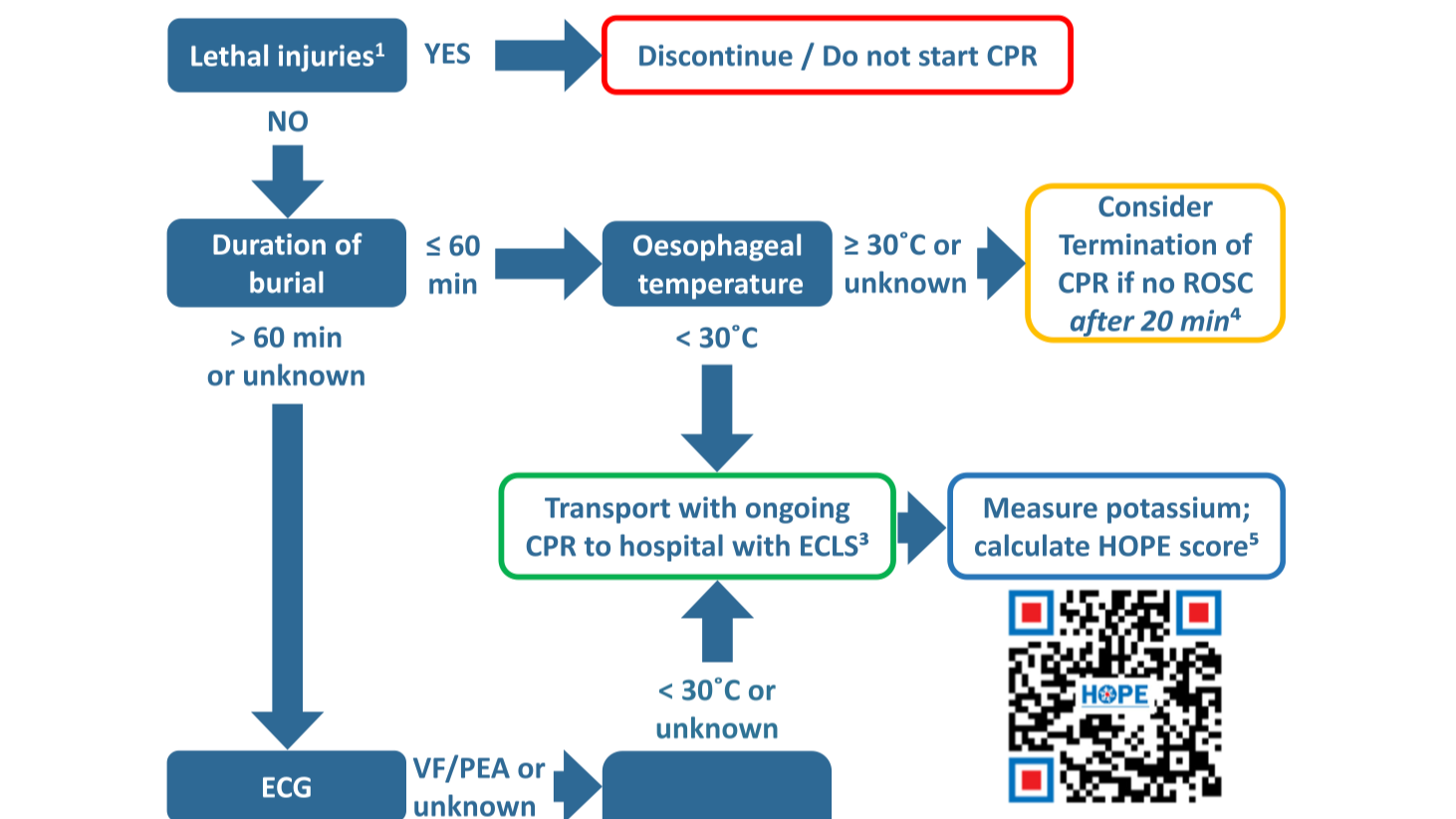
Asphyxia is the predominant cause of death in avalanche burial (65–100%), with trauma (5–29%) and hypothermia (0–4%) as less common etiologies, necessitating airway assessment and early rescue breaths for those without signs of life and burial <60 minutes.
Survival is strongly related to burial duration and airway patency; a burial duration <15 minutes has over 90% survival, while survival decreases rapidly thereafter, especially beyond 35–45 minutes, and is near zero with obstructed airway and asystole after >60 minutes.
Victims extricated after >60 minutes without signs of life but with a patent or unknown airway should be presumed to have suffered hypothermic cardiac arrest and should receive prolonged resuscitation and transport to ECLS-capable centers, unless core temperature excludes hypothermia.
Core temperature measurement (preferably esophageal in CA or intubated patients) is essential for triage in prolonged burials; a core temperature <30°C in victims without signs of life and with a patent airway should prompt resuscitation and ECLS consideration.
Presence of an air pocket significantly increases survival odds, especially in burials >15 minutes; however, even with an air pocket, severe asphyxia and hypercapnia can occur, and absence of an air pocket is associated with much lower survival.
Advanced ECG monitoring should be initiated as soon as possible in victims buried >60 minutes; ventricular fibrillation or PEA suggests possible hypothermic arrest, while asystole in the setting of prolonged burial and obstructed airway indicates poor prognosis and may preclude resuscitation.
Severe trauma, including head, thoracic, spinal, and pelvic injuries, as well as negative pressure pulmonary edema, are frequent in avalanche victims and should be managed per established trauma guidelines with spinal motion restriction and advanced trauma care.
In-hospital decision-making for ECLS rewarming in hypothermic avalanche cardiac arrest should utilize multivariable prognostic scores such as the HOPE score (preferably using the non-asphyxia scenario in cases of uncertainty), supplemented by potassium and temperature thresholds when appropriate.
https://www.resuscitationjournal.com/article/S0300-9572(23)00021-7/fulltext
Estimation of radiation-induced health hazards from a "dirty bomb"
This article examines the pathophysiology and clinical consequences of conventional and radiological (dirty bomb) explosions. Explosions generate rapid exothermic reactions resulting in high-pressure shockwaves and a fireball, which can disseminate hazardous particles, including radionuclides in the case of dirty bombs. The severity and distribution of injuries and contaminants are dictated by explosive yield, environmental conditions (notably, atmospheric stability), and particle characteristics.
Blast injuries are categorized as primary (shockwave effects, mainly on air-filled organs), secondary (trauma from projectiles), tertiary (injuries from bodily displacement), quaternary (burns and crushes), and quinary (effects from radiological, chemical, or biological contamination).
Confined-space detonations result in more severe thermal injuries and higher mortality. Radiological hazards arise from external irradiation (cloud or ground shine) and internal contamination (especially inhalation of fine particulate matter), with health risks—including malignancy and non-cancer mortality—increasing in a dose-dependent fashion and affected by nuclide kinetics.
Management principles emphasize immediate trauma triage and stabilization over radiation-specific concerns, as the majority of fatalities are due to mechanical and thermal trauma occurring at or near the time of detonation. Subsequent assessment for radiological exposure and internal contamination is essential, especially in dirty bomb events, given the potential for long-term health consequences.
Key Takeaways:Explosions yield multiple injury types—mechanical and, with dirty bombs, radiological—with primary focus in acute care on stabilization and trauma triage.Major radiological health risks include both external irradiation and internal contamination, with long-term increases in cancer and non-cancer morbidity.Injury and contaminant dispersion depend on explosive energy, environmental conditions, and particle size, making these factors critical in risk assessment.
Find Detailed questions on app.embllm.com
Managing bleeds on anticoagulant therapy
Bleeding remains the most significant and frequent complication of oral anticoagulant (OAC) therapy, impacting morbidity, mortality, and the risk of thromboembolic events if anticoagulation is interrupted.
While direct oral anticoagulants (DOACs) offer superior safety against intracranial bleeding compared to vitamin K antagonists (VKAs), they may present an increased risk of gastrointestinal bleeding. The use of combination antithrombotic therapy (e.g., OAC plus antiplatelet agents) heightens the bleeding risk, highlighting the need for individualized patient and regimen selection, along with regular reassessment using validated bleeding risk scores such as HAS-BLED and PRECISE-HBR. It is crucial to avoid unnecessary triple therapy, manage drug interactions, and implement routine gastroprotection for high-risk patients.
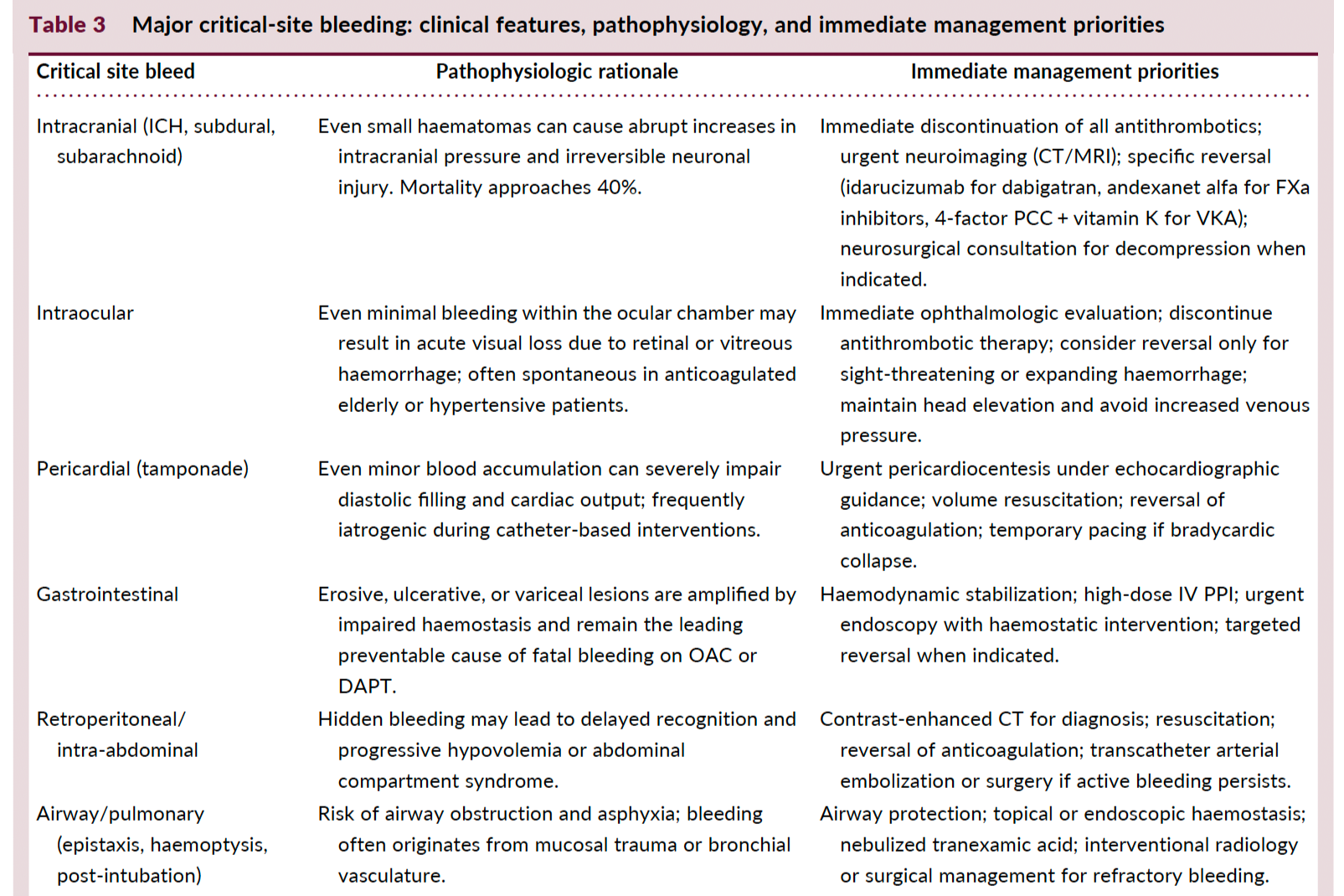
Hemodynamic instability or involvement of critical anatomical sites (e.g., intracranial, gastrointestinal) necessitates urgent stabilization, discontinuation of antithrombotics, targeted resuscitation, and, when indicated, anticoagulant reversal using drug-specific antidotes (idarucizumab for dabigatran, andexanet alfa or PCC for FXa inhibitors, vitamin K + PCC for VKAs).
Early intervention with multidisciplinary involvement enhances outcomes. Restarting OAC after major bleeding should be prioritized once hemostasis and source control are achieved, balancing the patient-specific thrombotic versus bleeding risk, and considering dose reduction or agent change where appropriate.
Minor bleeding is common but rarely requires hospitalization or cessation of therapy. Management is primarily supportive, focusing on local measures, correction of reversible risk factors, and avoiding unnecessary OAC interruption.
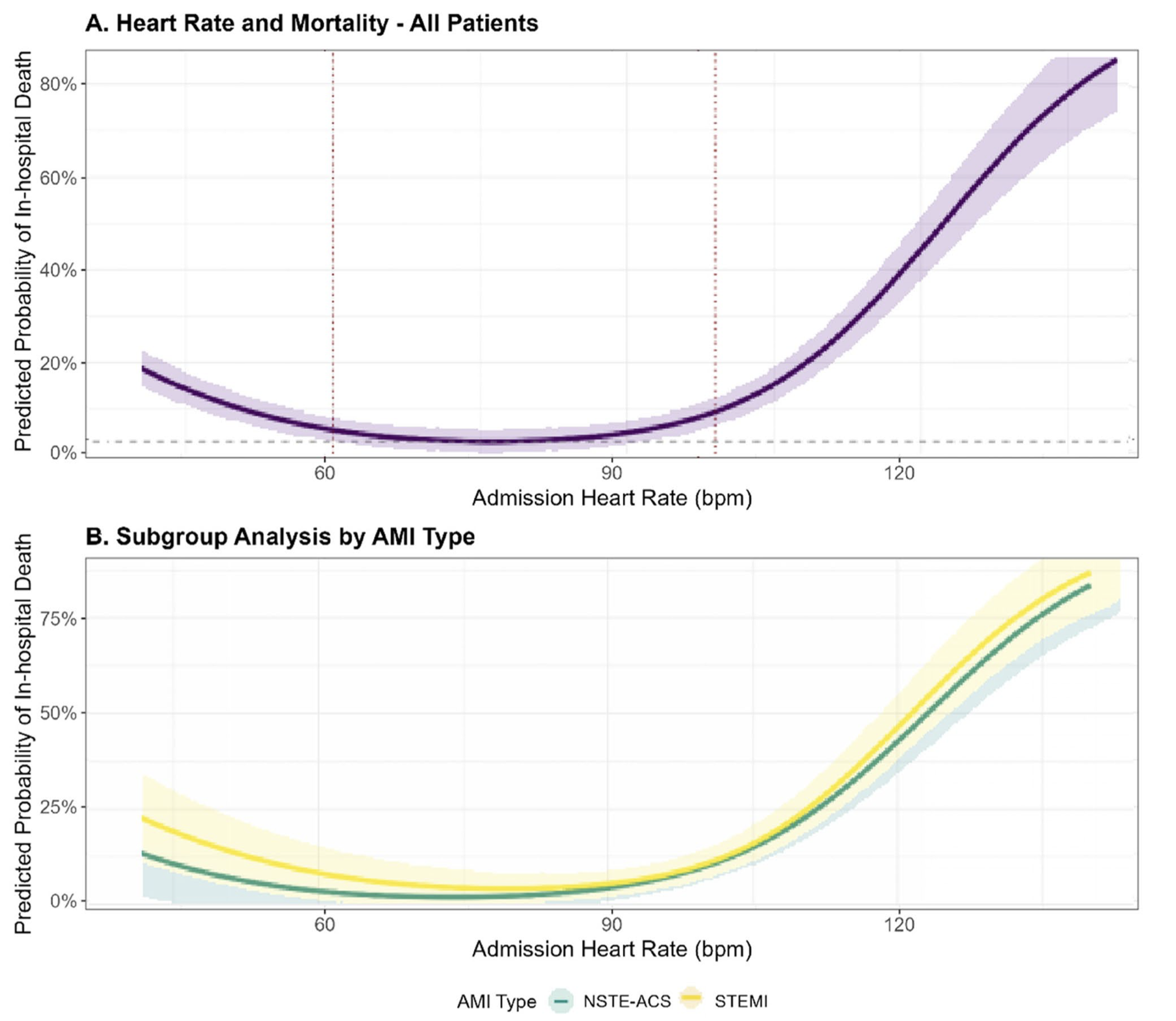
Admission heart rate and in-hospital mortality in acute myocardial infarction: a contemporary analysis of the MIMIC-III cohort
Admission heart rate (HR) in patients with acute myocardial infarction (AMI) exhibits a U-shaped association with in-hospital mortality, with both bradycardia (<60 bpm) and tachycardia (≥100 bpm) conferring significantly increased risk compared to the reference range (60–99 bpm).
After multivariable adjustment—including for age, sex, Killip class, systolic blood pressure, reperfusion therapy, comorbidities, and initial laboratory values—HR <60 bpm was associated with a 58% higher odds (aOR 1.58, 95% CI 1.02–2.45) and HR ≥100 bpm with a 145% higher odds (aOR 2.45, 95% CI 1.56–3.85) of in-hospital death.
The U-shaped HR–mortality relationship remained robust even after sensitivity analyses accounting for early mortality (<24 h).
This relationship is more pronounced in STEMI patients than in those with NSTE-ACS, with the steepest rise in mortality observed in STEMI patients presenting with tachycardia, and a somewhat greater impact of bradycardia in NSTE-ACS.
The optimal HR nadir for lowest in-hospital mortality differed by AMI subtype (≈78 bpm in STEMI and ≈72 bpm in NSTE-ACS), indicating a need for subtype-specific monitoring and intervention thresholds.
No significant effect modification by age, sex, hypertension, or early β-blocker use was observed, suggesting that the prognostic value of admission HR is consistent across these subpopulations.
Admission HR reflects integrated physiological responses, including autonomic tone, hemodynamic stress, and underlying conduction system disturbances, and thus serves as a rapid and practical risk stratification tool at the bedside.
Clinical implication: Patients presenting with admission HR outside the 60–99 bpm range MAY warrant prompt hemodynamic stabilization and closer monitoring, and prospective studies are needed to determine whether targeted HR normalization improves short-term outcomes in AMI.
How Physicians Can Stay Up to Date With the Latest Evidence-Based Medicine
Keeping up with evidence-based medicine (EBM) has never been more important—or more challenging. Thousands of peer-reviewed articles are published every week, clinical guidelines evolve rapidly, and new diagnostic and therapeutic approaches continually emerge. For busy physicians, staying current requires efficient, evidence-driven strategies.
Below are proven methods physicians use to remain up to date, with an emphasis on tools that reduce cognitive and time burden—such as EMBLLM.
1. Focus on High-Yield Medical Journals
Leading journals such as NEJM, JAMA, The Lancet, and specialty-specific publications remain foundational sources of new evidence. However, attempting to read every article is unrealistic and expensive.
Physicians benefit most from identifying high-yield, practice-changing studies, including randomized controlled trials, systematic reviews, and meta-analyses—an approach that mirrors how EMBLLM selects content for its quizzes.
2. Use PubMed With Purpose
PubMed is the most comprehensive database of peer-reviewed biomedical literature, but its volume can be overwhelming. Strategic use is key.
Effective approaches include:
Filtering for recent publications
Prioritizing clinical trials and guideline-informing studies
Focusing on articles with clear implications for patient care
EMBLLM applies this same methodology by reviewing PubMed regularly and selecting available, high-yield peer-reviewed articles that are most relevant to clinical practice.
3. Rely on Updated Clinical Guidelines
Professional society guidelines synthesize large bodies of evidence into actionable recommendations. Reviewing guideline updates is often more efficient than reading individual studies.
EMBLLM complements this process by reinforcing the underlying evidence behind guideline recommendations, helping physicians understand why practices change—not just that they have changed.
4. Participate in CME and Conferences
CME activities and conferences remain valuable for learning about emerging evidence and landmark trials. However, retention can be limited without reinforcement.
Tools like EMBLLM extend learning beyond conferences by transforming recent peer-reviewed research into interactive, question-based learning, helping physicians retain and apply new knowledge more effectively.
5. Engage in Active Learning Through Question-Based Review
Active recall has been shown to significantly improve knowledge retention compared to passive reading. Question-based learning encourages physicians to identify gaps, challenge assumptions, and apply evidence in clinical scenarios.
EMBLLM leverages this approach by converting current scientific literature into quizzes grounded in peer-reviewed research, reinforcing evidence-based decision-making in a time-efficient format.
6. Build a Sustainable, Time-Efficient Routine
Consistency matters more than volume. Even short, regular learning sessions can have a meaningful impact over time.
By curating high-yield PubMed articles and presenting them as concise quizzes, EMBLLM allows physicians to stay current without needing to sift through hundreds of publications, making evidence-based learning more sustainable in everyday practice.
Conclusion
Staying current with evidence-based medicine is a professional responsibility—but it does not require reading every paper or attending every conference. By combining selective journal review, guideline monitoring, CME participation, and modern tools like EMBLLM, physicians can efficiently stay informed while maintaining clinical focus.
EMBLLM supports this process by reviewing PubMed, selecting high-yield peer-reviewed articles, and translating them into engaging, clinically relevant quizzes—helping physicians keep pace with the rapidly evolving medical literature.
How does EMBLLM ensure the quizzes are based on the most recent peer-reviewed scientific papers?
How does EMBLLM ensure the quizzes are based on the most recent peer-reviewed scientific papers?
EMBLLM ensures that all quizzes are built on the most recent and relevant peer-reviewed scientific literature by conducting thorough reviews of PubMed and other reputable scientific databases. We focus on selecting high-yield articles that provide the most accurate and up-to-date information in the field. Our team carefully curates content from these sources to ensure that each quiz reflects the latest advancements in medical science and aligns with current best practices.
Integration of Language Models: EMBLLM utilizes language models, to review the available literature and curate targeted information from each article for our users.
Dynamic Benchmarking: To maintain the relevance and accuracy of its quizzes, EMBLLM incorporates dynamic evaluation benchmarks to ensure we have covered all the necessary topics for a speciality.
Expert Supervision and Validation: While large language models can generate multiple-choice questions, studies have shown that a significant portion may contain flaws or errors. Therefore, EMBLLM emphasizes the importance of expert supervision in the question-generation process to ensure the accuracy and quality of the quizzes. (pubmed.ncbi.nlm.nih.gov)
By combining specialized language models, dynamic benchmarking, and expert oversight, EMBLLM strives to provide quizzes that reflect the most current and reliable scientific knowledge.

How Physicians Can Stay Up to Date on the Latest Medical Research
Medical knowledge is expanding at an unprecedented pace. Every week, hundreds of new studies are published across clinical specialties, making it increasingly challenging for physicians to stay current while managing busy practices and personal lives. Fortunately, there are several effective ways to keep up with the latest research without feeling overwhelmed.
Below are practical, realistic strategies physicians can use to stay informed about new journal publications and emerging evidence.
1. Reading Peer-Reviewed Journals Directly
Traditional medical journals remain the gold standard for new research. Journals such as NEJM, JAMA, The Lancet, and specialty-specific publications provide rigorous, peer-reviewed studies that shape clinical practice.
Best practices:
Focus on a short list of high-impact journals relevant to your specialty
Read abstracts first to decide whether full articles are clinically relevant
Set aside brief, scheduled time blocks for review
Limitations:
Time constraints often make it difficult to read full articles regularly, especially lengthy original research.
2. Journal Email Alerts and Table of Contents (TOC) Updates
Most journals offer free email alerts that notify subscribers when new issues or articles are published.
Why this works:
Automatically delivers updates to your inbox
Helps you scan titles and abstracts quickly
Reduces the need for manual searching
This method is ideal for identifying key papers without committing to reading every publication in full.
3. Clinical Summaries and Evidence-Based Digests
Many platforms curate and summarize new research into concise, clinically relevant insights.
Benefits:
Saves time by distilling key findings
Emphasizes clinical applicability
Helps identify practice-changing evidence
Summaries are especially helpful for physicians who want actionable takeaways rather than exhaustive statistical analysis.
4. CME Activities Based on New Research
Continuing Medical Education (CME) is increasingly built around newly published studies and updated guidelines.
Advantages:
Keeps you current while earning required CME credits
Often focuses on guideline-changing or high-impact research
Structured learning with expert interpretation
This approach allows physicians to stay up to date while meeting licensure and certification requirements.
5. App-Based Research and Learning Platforms
App-based platforms have become one of the most efficient ways for physicians to keep up with journal literature.
Why app-based learning stands out:
Push notifications highlight important new studies
Short, focused summaries fit into busy schedules
Accessible anytime — between patients or during breaks
Enables learning without sacrificing evenings or family time
Rather than searching through multiple journals, physicians can rely on curated, specialty-specific content delivered directly to their phones.
6. Podcasts and Audio Summaries
Medical podcasts that review and discuss new research offer another flexible option.
Ideal for:
Commutes or workouts
Passive learning during daily routines
While podcasts are a great supplement, they are best paired with other methods to ensure comprehensive coverage.
7. Professional Societies and Guidelines
Specialty societies frequently review emerging research and incorporate findings into clinical guidelines.
Benefits:
Expert interpretation of evidence
Clear recommendations for practice
Helps bridge the gap between research and real-world application
Following society updates ensures you’re aware of major changes that affect patient care.
Choosing the Right Approach
No single method is sufficient on its own. Most physicians benefit from combining:
Journal alerts for awareness
App-based summaries for efficiency
CME activities for structured learning
This layered approach allows you to stay informed without information overload.
Final Thoughts
Staying current with medical research is essential — but it doesn’t have to be overwhelming. By using modern tools like curated summaries, CME-based learning, and app-based platforms, physicians can keep up with the latest journal publications on their own schedule. The result is better patient care, professional confidence, and a sustainable way to stay informed in an ever-evolving field of medicine.

Navigating Continuing Medical Education Requirements for Physicians: A State-by-State Guide
For licensed physicians in the United States, maintaining licensure isn’t just about passing exams and completing residency — it also requires staying current through Continuing Medical Education (CME). Whether you practice in one state or several, knowing how each state’s CME requirements work can save time, headache, and potential compliance issues.
Why CME Matters
Every state medical board sets CME requirements as part of physician licensure renewal. These requirements vary widely — from the number of credits needed to the topics that must be covered — and often overlap with national requirements, such as maintenance of certification (MOC) from specialty boards. Understanding these expectations helps you stay compliant, deliver better care, and avoid license issues.
CME Requirements Across the States
Each state sets its own CME credit requirements, renewal cycles, and content mandates. Here’s a snapshot of how those vary:
Alabama – 25/year
Alaska – 25/year
Arizona – 40/2 years
Arkansas – 20/year
California – 50/2 years
Colorado — has no CME requirements for physicians.
Connecticut — 50/2 years
Delaware – 40/2 years
District of Columbia — 50/2 years
Florida — 40/2 years
Georgia — 40/2 years
Hawaii — 40/2 years
Idaho — 40/2 years
Illinois — 150/3 years
Indiana —2/2 years
Iowa — 40/2 years
Kansas — 50/year
Kentucky — 60/3 years
Louisiana — 20/year
Maine — 100/2 years
Maryland — 50/2 years
Massachusetts — 50/2 years
Michigan — 150/3 years
Minnesota – —75/3 year
Mississippi — 40/2 years
Missouri – 50/2 years
Montana — no CME requirement
Nebraska — 50/2 years
Nevada — 40/2 years
New Hampshire — 100/2 years
New Jersey — 100/2 years
New Mexico — 75/3 years
New York — no CME requirement
North Carolina — 60/3 years
North Dakota — 60/3 years
Ohio — 100/2 years
Oklahoma — 60/3 years
Oregon — 60/2 years
Pennsylvania — 100/2 years
Rhode Island — 40/2 years
South Carolina — 40/2 years
South Dakota — no CME requirement
Tennessee — 40/2 years
Texas — 48/2 years
Utah — 40/2 years
Vermont — 30/2 years
Virginia — 60/2 years
Washington — 200/4 years
West Virginia — 50/2 years
Wisconsin — 30/2 years
Wyoming — 60/3 years
Quick Tip: Some states require specific topic content — such as pain management, controlled substance prescribing, patient safety, or ethics — in addition to general CME credits. These content mandates can vary by state and by licensure cycle.
How National and State Requirements Interact
Physicians often hold multiple licenses or are board-certified in a specialty. In these cases:
State CME requirements apply to each license you hold.
National standards (like MOC from boards such as ABMS) may have separate CME or professional development expectations.
Some platforms — like the AMA Ed Hub — can help track CME requirements for multiple states and specialties, making it easier to meet both state and national requirements in one place. AMA Ed Hub
Practical Tips to Stay Compliant
Here are some strategies to stay on top of CME requirements without stress:
📍 Track Requirements Early and Often
Don’t wait until renewal season. Keep a checklist of each state/license’s required hours and any specific content topics.
📍 Centralize Your CME Records
Maintain a digital folder of certificates and dates. Many licensing boards perform random audits — having easy access to your records will save time and anxiety.
📍 Align CME with Practice Needs
Whenever possible, choose CME activities that serve multiple purposes: state licensure, specialty certification/MOC, and your own clinical growth.
Final Thoughts
Physician CME requirements in the United States are state-specific and multifaceted. Some states have high credit demands, others require specific topics, and a few don’t require general CME at all. However, all physicians benefit from proactive tracking and strategic CME planning.
Staying compliant doesn’t have to be a chore — with the right tools and planning, you can meet both your state and national CME obligations efficiently, and continue delivering excellent patient care without last-minute scrambling.

Exploring the Different Ways Physicians Can Earn CME
It All Begins Here
Continuing Medical Education (CME) is an essential part of a physician’s professional life. Medicine evolves rapidly, and staying current with new research, guidelines, and best practices is critical for providing high-quality patient care. Fortunately, physicians today have more options than ever for earning CME—each with its own benefits and challenges. Let’s explore the most common formats and why app-based learning is increasingly becoming the preferred choice.
1. Conferences and Live Events
Medical conferences have long been a traditional way for physicians to earn CME. These events offer live lectures, hands-on workshops, and opportunities to network with peers and experts in the field.
Pros:
Direct interaction with experts
Networking and professional collaboration
Immersive learning environment
Cons:
Requires travel and time away from work and family
Expensive registration, lodging, and transportation
Fixed schedules that may not fit a physician’s routine
While conferences can be valuable, the time commitment often makes them difficult to attend regularly.
2. Self-Study Materials
Self-study options include textbooks, journals, online articles, and recorded lectures. These materials allow physicians to learn independently and often at a lower cost.
Pros:
Flexible pacing
Can be accessed from anywhere
Wide range of topics available
Cons:
Requires dedicated, uninterrupted time
Can feel passive or less engaging
Easy to postpone amid a busy schedule
Self-study works well for motivated learners, but it can be challenging to consistently carve out focused time.
3. Podcasts
Medical podcasts have gained popularity as a convenient way to stay informed. Physicians can listen while commuting, exercising, or doing daily tasks.
Pros:
Easy to fit into daily routines
Engaging and conversational format
Great for staying up to date on trends
Cons:
Limited interactivity
Not all podcasts offer accredited CME
Learning depth may vary
Podcasts are an excellent supplement, but they may not always provide comprehensive CME coverage.
4. App-Based Learning: The Most Convenient Option
App-based CME learning has emerged as the most practical and physician-friendly option. These platforms are designed specifically for busy clinicians, offering short, focused learning modules that can be completed anytime, anywhere.
Why app-based learning stands out:
Ultimate flexibility: Learn during breaks, between patients, or whenever time allows
On-demand access: No fixed schedules or deadlines
Bite-sized content: Easy to absorb without feeling overwhelmed
Protects family time: Learning fits into a physician’s life rather than competing with personal commitments
Unlike conferences or scheduled sessions, app-based CME allows physicians to stay current without sacrificing evenings, weekends, or family time. This balance is especially important in a profession where burnout is already a concern.
Conclusion
Physicians have multiple ways to earn CME, from traditional conferences to modern digital formats. While each method has value, app-based learning offers unmatched convenience, flexibility, and efficiency. By allowing doctors to learn on their own time—without travel or rigid schedules—app-based CME supports both professional growth and personal well-being. In today’s demanding healthcare environment, that balance makes all the difference.