Care of Avalanche Patients
Asphyxia is the predominant cause of death in avalanche burial (65–100%), with trauma (5–29%) and hypothermia (0–4%) as less common etiologies, necessitating airway assessment and early rescue breaths for those without signs of life and burial <60 minutes.
Survival is strongly related to burial duration and airway patency; a burial duration <15 minutes has over 90% survival, while survival decreases rapidly thereafter, especially beyond 35–45 minutes, and is near zero with obstructed airway and asystole after >60 minutes.
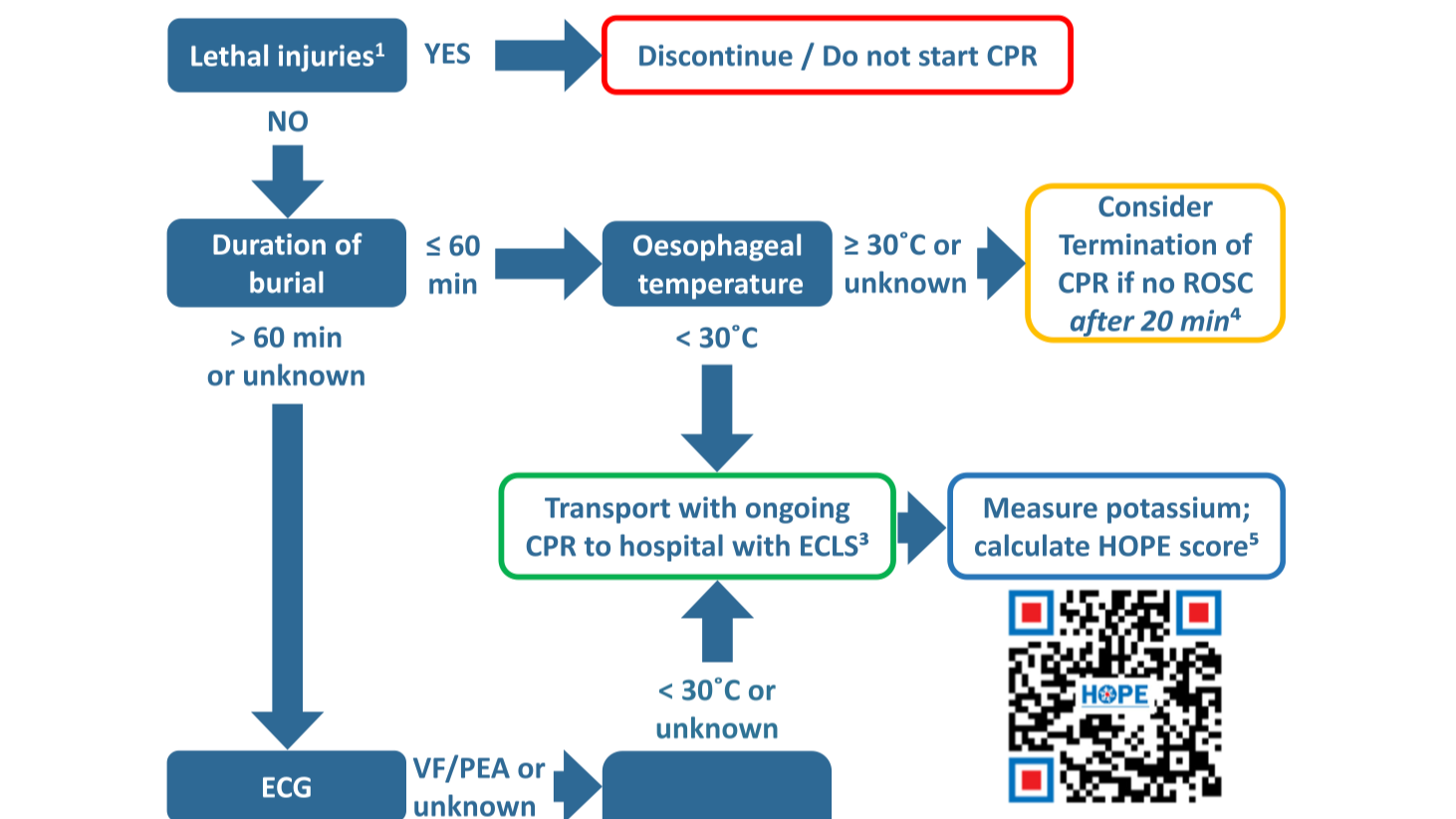
Victims extricated after >60 minutes without signs of life but with a patent or unknown airway should be presumed to have suffered hypothermic cardiac arrest and should receive prolonged resuscitation and transport to ECLS-capable centers, unless core temperature excludes hypothermia.
Core temperature measurement (preferably esophageal in CA or intubated patients) is essential for triage in prolonged burials; a core temperature <30°C in victims without signs of life and with a patent airway should prompt resuscitation and ECLS consideration.
Presence of an air pocket significantly increases survival odds, especially in burials >15 minutes; however, even with an air pocket, severe asphyxia and hypercapnia can occur, and absence of an air pocket is associated with much lower survival.
Advanced ECG monitoring should be initiated as soon as possible in victims buried >60 minutes; ventricular fibrillation or PEA suggests possible hypothermic arrest, while asystole in the setting of prolonged burial and obstructed airway indicates poor prognosis and may preclude resuscitation.
Severe trauma, including head, thoracic, spinal, and pelvic injuries, as well as negative pressure pulmonary edema, are frequent in avalanche victims and should be managed per established trauma guidelines with spinal motion restriction and advanced trauma care.
In-hospital decision-making for ECLS rewarming in hypothermic avalanche cardiac arrest should utilize multivariable prognostic scores such as the HOPE score (preferably using the non-asphyxia scenario in cases of uncertainty), supplemented by potassium and temperature thresholds when appropriate.
https://www.resuscitationjournal.com/article/S0300-9572(23)00021-7/fulltext