Estimation of radiation-induced health hazards from a "dirty bomb"
This article examines the pathophysiology and clinical consequences of conventional and radiological (dirty bomb) explosions. Explosions generate rapid exothermic reactions resulting in high-pressure shockwaves and a fireball, which can disseminate hazardous particles, including radionuclides in the case of dirty bombs. The severity and distribution of injuries and contaminants are dictated by explosive yield, environmental conditions (notably, atmospheric stability), and particle characteristics.
Blast injuries are categorized as primary (shockwave effects, mainly on air-filled organs), secondary (trauma from projectiles), tertiary (injuries from bodily displacement), quaternary (burns and crushes), and quinary (effects from radiological, chemical, or biological contamination).
Confined-space detonations result in more severe thermal injuries and higher mortality. Radiological hazards arise from external irradiation (cloud or ground shine) and internal contamination (especially inhalation of fine particulate matter), with health risks—including malignancy and non-cancer mortality—increasing in a dose-dependent fashion and affected by nuclide kinetics.
Management principles emphasize immediate trauma triage and stabilization over radiation-specific concerns, as the majority of fatalities are due to mechanical and thermal trauma occurring at or near the time of detonation. Subsequent assessment for radiological exposure and internal contamination is essential, especially in dirty bomb events, given the potential for long-term health consequences.
Key Takeaways:Explosions yield multiple injury types—mechanical and, with dirty bombs, radiological—with primary focus in acute care on stabilization and trauma triage.Major radiological health risks include both external irradiation and internal contamination, with long-term increases in cancer and non-cancer morbidity.Injury and contaminant dispersion depend on explosive energy, environmental conditions, and particle size, making these factors critical in risk assessment.
Find Detailed questions on app.embllm.com
Managing bleeds on anticoagulant therapy
Bleeding remains the most significant and frequent complication of oral anticoagulant (OAC) therapy, impacting morbidity, mortality, and the risk of thromboembolic events if anticoagulation is interrupted.
While direct oral anticoagulants (DOACs) offer superior safety against intracranial bleeding compared to vitamin K antagonists (VKAs), they may present an increased risk of gastrointestinal bleeding. The use of combination antithrombotic therapy (e.g., OAC plus antiplatelet agents) heightens the bleeding risk, highlighting the need for individualized patient and regimen selection, along with regular reassessment using validated bleeding risk scores such as HAS-BLED and PRECISE-HBR. It is crucial to avoid unnecessary triple therapy, manage drug interactions, and implement routine gastroprotection for high-risk patients.
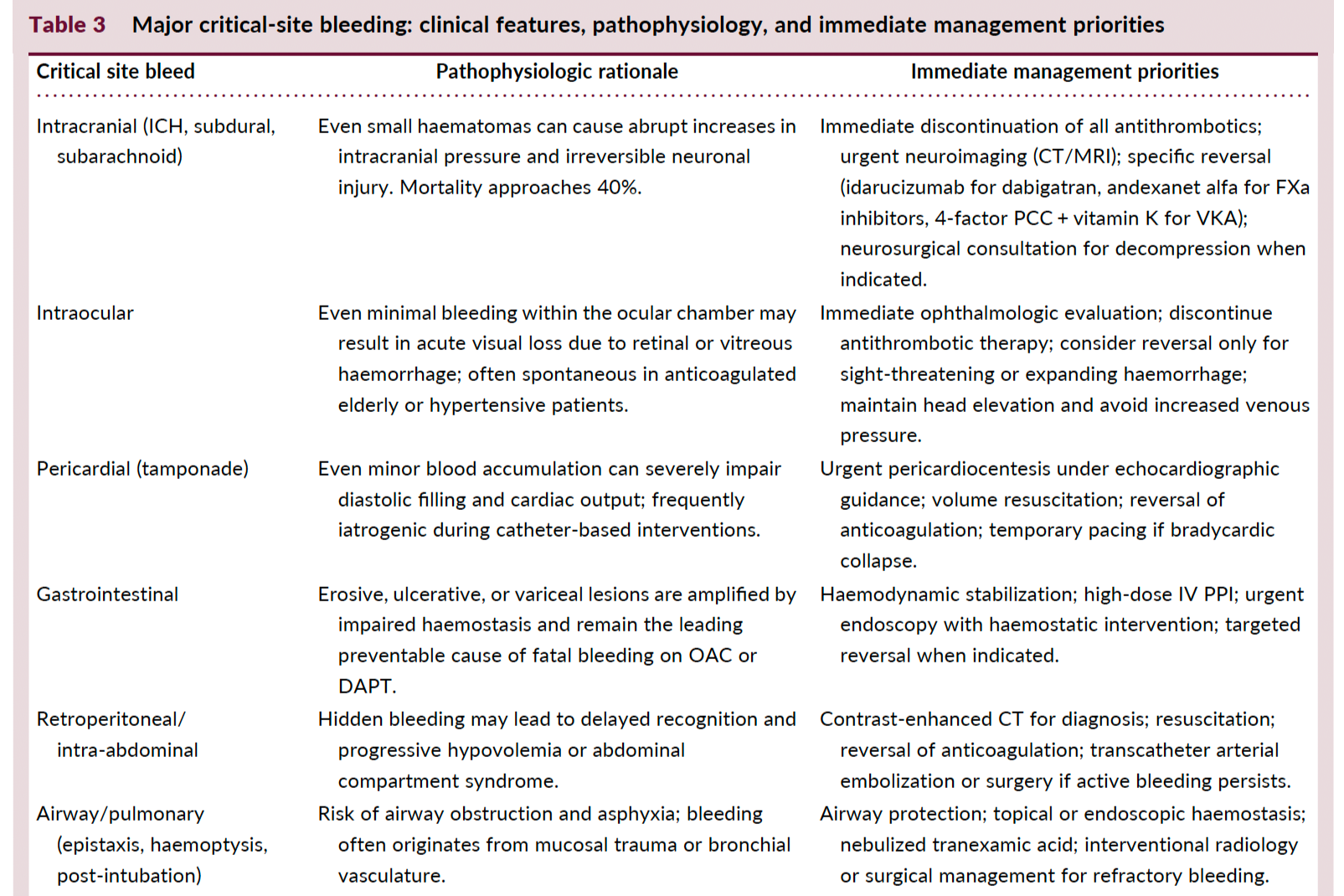
Hemodynamic instability or involvement of critical anatomical sites (e.g., intracranial, gastrointestinal) necessitates urgent stabilization, discontinuation of antithrombotics, targeted resuscitation, and, when indicated, anticoagulant reversal using drug-specific antidotes (idarucizumab for dabigatran, andexanet alfa or PCC for FXa inhibitors, vitamin K + PCC for VKAs).
Early intervention with multidisciplinary involvement enhances outcomes. Restarting OAC after major bleeding should be prioritized once hemostasis and source control are achieved, balancing the patient-specific thrombotic versus bleeding risk, and considering dose reduction or agent change where appropriate.
Minor bleeding is common but rarely requires hospitalization or cessation of therapy. Management is primarily supportive, focusing on local measures, correction of reversible risk factors, and avoiding unnecessary OAC interruption.