Peripheral Artery Disease: Review
Peripheral arterial disease (PAD) is primarily driven by atherosclerosis related to hypertension, diabetes mellitus, hyperlipidemia, and smoking, with microvascular and endothelial dysfunction exacerbating disease progression and complications.
Duplex ultrasound (DUS) is recommended as the first-line, non-invasive imaging modality for PAD diagnosis and surveillance, offering high sensitivity and specificity in most arterial segments while avoiding contrast or radiation exposure, particularly beneficial for patients with renal impairment.
Optimal medical management for PAD includes aggressive risk factor modification (smoking cessation, statin therapy regardless of baseline LDL, antihypertensive therapy, antithrombotic agents—preferably single antiplatelet, and glycemic control in diabetes), with strong evidence supporting supervised exercise therapy for symptomatic relief in claudication.
Endovascular interventions, such as balloon angioplasty (including drug-coated and lithotripsy balloons) and stent placement (preferably nitinol or covered stents for specific lesions), are generally preferred over surgical revascularization for aortoiliac and femoropopliteal disease due to lower morbidity, comparable limb salvage, and improved quality of life outcomes.
Surgical bypass remains the gold standard for complete femoropopliteal occlusions and long or complex lesions, but is associated with higher perioperative morbidity and mortality, making endovascular-first strategy preferable in most other anatomical locations or high-risk patients.
In endovascular therapy, advancements such as 2D fusion imaging and retrograde re-entry catheters have significantly reduced radiation and contrast loads while increasing technical success rates, particularly for chronic total occlusions and challenging anatomy.The choice of revascularization strategy must be individualized based on anatomic lesion (TASC II classification), patient comorbidities and surgical risk, with endovascular-first approaches supported for most lesions except for certain complex infrapopliteal or common femoral artery diseases where open surgery or endarterectomy may yield superior long-term patency.
earn CME at app.embllm.com
This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Scimple Education, LLC, and EMBLLM, LLC. Scimple Education, LLC is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Scimple Education, LLC designates this Enduring Material for a maximum of 24.0 AMA PRA Category 1 Credits™ for physicians. Physicians should claim only the credit commensurate with the extent of their participation in this activity.
Estimation of radiation-induced health hazards from a "dirty bomb"
This article examines the pathophysiology and clinical consequences of conventional and radiological (dirty bomb) explosions. Explosions generate rapid exothermic reactions resulting in high-pressure shockwaves and a fireball, which can disseminate hazardous particles, including radionuclides in the case of dirty bombs. The severity and distribution of injuries and contaminants are dictated by explosive yield, environmental conditions (notably, atmospheric stability), and particle characteristics.
Blast injuries are categorized as primary (shockwave effects, mainly on air-filled organs), secondary (trauma from projectiles), tertiary (injuries from bodily displacement), quaternary (burns and crushes), and quinary (effects from radiological, chemical, or biological contamination).
Confined-space detonations result in more severe thermal injuries and higher mortality. Radiological hazards arise from external irradiation (cloud or ground shine) and internal contamination (especially inhalation of fine particulate matter), with health risks—including malignancy and non-cancer mortality—increasing in a dose-dependent fashion and affected by nuclide kinetics.
Management principles emphasize immediate trauma triage and stabilization over radiation-specific concerns, as the majority of fatalities are due to mechanical and thermal trauma occurring at or near the time of detonation. Subsequent assessment for radiological exposure and internal contamination is essential, especially in dirty bomb events, given the potential for long-term health consequences.
Key Takeaways:Explosions yield multiple injury types—mechanical and, with dirty bombs, radiological—with primary focus in acute care on stabilization and trauma triage.Major radiological health risks include both external irradiation and internal contamination, with long-term increases in cancer and non-cancer morbidity.Injury and contaminant dispersion depend on explosive energy, environmental conditions, and particle size, making these factors critical in risk assessment.
Find Detailed questions on app.embllm.com
Admission heart rate and in-hospital mortality in acute myocardial infarction: a contemporary analysis of the MIMIC-III cohort
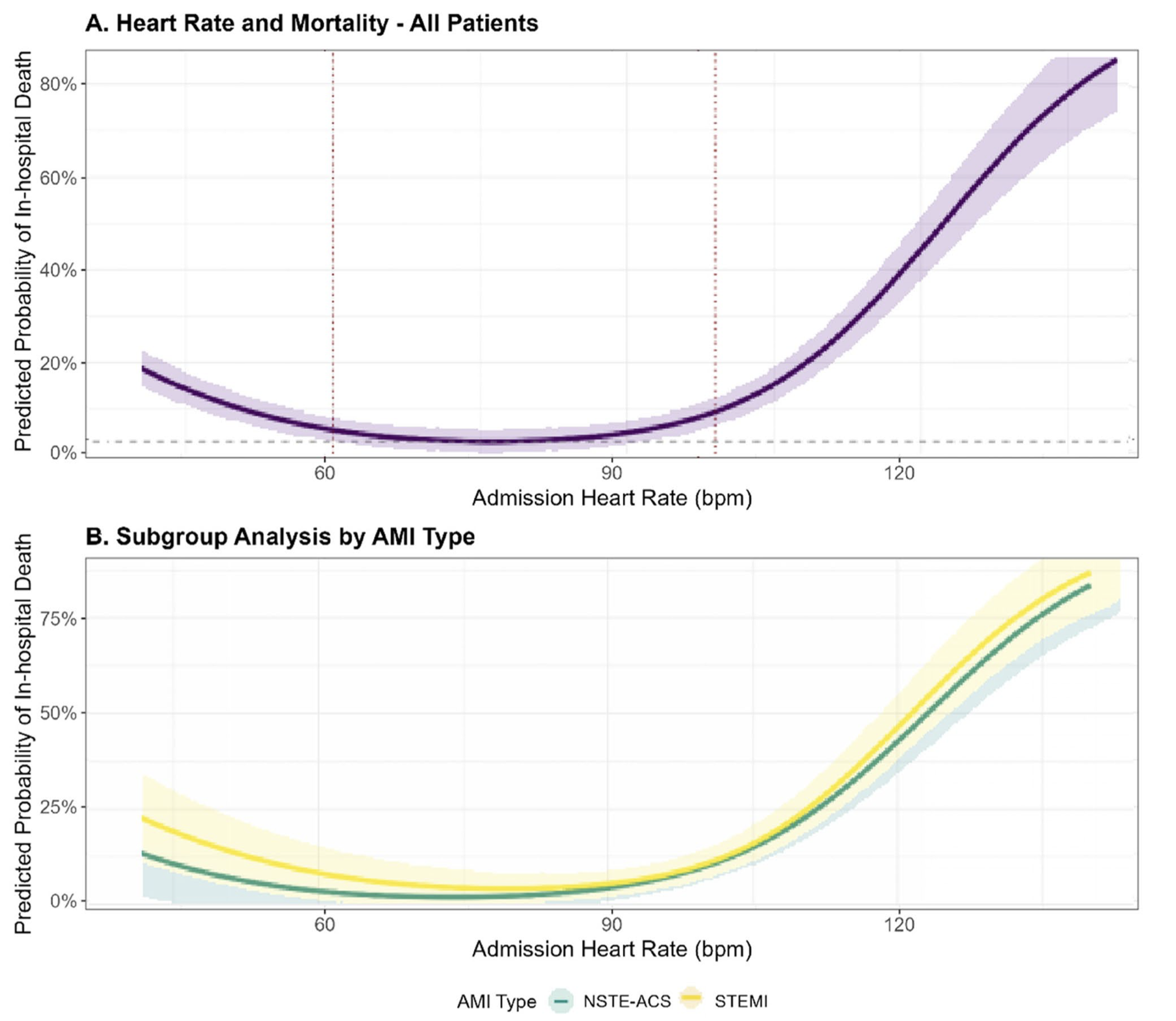
Admission heart rate (HR) in patients with acute myocardial infarction (AMI) exhibits a U-shaped association with in-hospital mortality, with both bradycardia (<60 bpm) and tachycardia (≥100 bpm) conferring significantly increased risk compared to the reference range (60–99 bpm).
After multivariable adjustment—including for age, sex, Killip class, systolic blood pressure, reperfusion therapy, comorbidities, and initial laboratory values—HR <60 bpm was associated with a 58% higher odds (aOR 1.58, 95% CI 1.02–2.45) and HR ≥100 bpm with a 145% higher odds (aOR 2.45, 95% CI 1.56–3.85) of in-hospital death.
The U-shaped HR–mortality relationship remained robust even after sensitivity analyses accounting for early mortality (<24 h).
This relationship is more pronounced in STEMI patients than in those with NSTE-ACS, with the steepest rise in mortality observed in STEMI patients presenting with tachycardia, and a somewhat greater impact of bradycardia in NSTE-ACS.
The optimal HR nadir for lowest in-hospital mortality differed by AMI subtype (≈78 bpm in STEMI and ≈72 bpm in NSTE-ACS), indicating a need for subtype-specific monitoring and intervention thresholds.
No significant effect modification by age, sex, hypertension, or early β-blocker use was observed, suggesting that the prognostic value of admission HR is consistent across these subpopulations.
Admission HR reflects integrated physiological responses, including autonomic tone, hemodynamic stress, and underlying conduction system disturbances, and thus serves as a rapid and practical risk stratification tool at the bedside.
Clinical implication: Patients presenting with admission HR outside the 60–99 bpm range MAY warrant prompt hemodynamic stabilization and closer monitoring, and prospective studies are needed to determine whether targeted HR normalization improves short-term outcomes in AMI.