Peripheral Artery Disease: Review
Peripheral arterial disease (PAD) is primarily driven by atherosclerosis related to hypertension, diabetes mellitus, hyperlipidemia, and smoking, with microvascular and endothelial dysfunction exacerbating disease progression and complications.
Duplex ultrasound (DUS) is recommended as the first-line, non-invasive imaging modality for PAD diagnosis and surveillance, offering high sensitivity and specificity in most arterial segments while avoiding contrast or radiation exposure, particularly beneficial for patients with renal impairment.
Optimal medical management for PAD includes aggressive risk factor modification (smoking cessation, statin therapy regardless of baseline LDL, antihypertensive therapy, antithrombotic agents—preferably single antiplatelet, and glycemic control in diabetes), with strong evidence supporting supervised exercise therapy for symptomatic relief in claudication.
Endovascular interventions, such as balloon angioplasty (including drug-coated and lithotripsy balloons) and stent placement (preferably nitinol or covered stents for specific lesions), are generally preferred over surgical revascularization for aortoiliac and femoropopliteal disease due to lower morbidity, comparable limb salvage, and improved quality of life outcomes.
Surgical bypass remains the gold standard for complete femoropopliteal occlusions and long or complex lesions, but is associated with higher perioperative morbidity and mortality, making endovascular-first strategy preferable in most other anatomical locations or high-risk patients.
In endovascular therapy, advancements such as 2D fusion imaging and retrograde re-entry catheters have significantly reduced radiation and contrast loads while increasing technical success rates, particularly for chronic total occlusions and challenging anatomy.The choice of revascularization strategy must be individualized based on anatomic lesion (TASC II classification), patient comorbidities and surgical risk, with endovascular-first approaches supported for most lesions except for certain complex infrapopliteal or common femoral artery diseases where open surgery or endarterectomy may yield superior long-term patency.
earn CME at app.embllm.com
This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Scimple Education, LLC, and EMBLLM, LLC. Scimple Education, LLC is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Scimple Education, LLC designates this Enduring Material for a maximum of 24.0 AMA PRA Category 1 Credits™ for physicians. Physicians should claim only the credit commensurate with the extent of their participation in this activity.
Managing bleeds on anticoagulant therapy
Bleeding remains the most significant and frequent complication of oral anticoagulant (OAC) therapy, impacting morbidity, mortality, and the risk of thromboembolic events if anticoagulation is interrupted.
While direct oral anticoagulants (DOACs) offer superior safety against intracranial bleeding compared to vitamin K antagonists (VKAs), they may present an increased risk of gastrointestinal bleeding. The use of combination antithrombotic therapy (e.g., OAC plus antiplatelet agents) heightens the bleeding risk, highlighting the need for individualized patient and regimen selection, along with regular reassessment using validated bleeding risk scores such as HAS-BLED and PRECISE-HBR. It is crucial to avoid unnecessary triple therapy, manage drug interactions, and implement routine gastroprotection for high-risk patients.
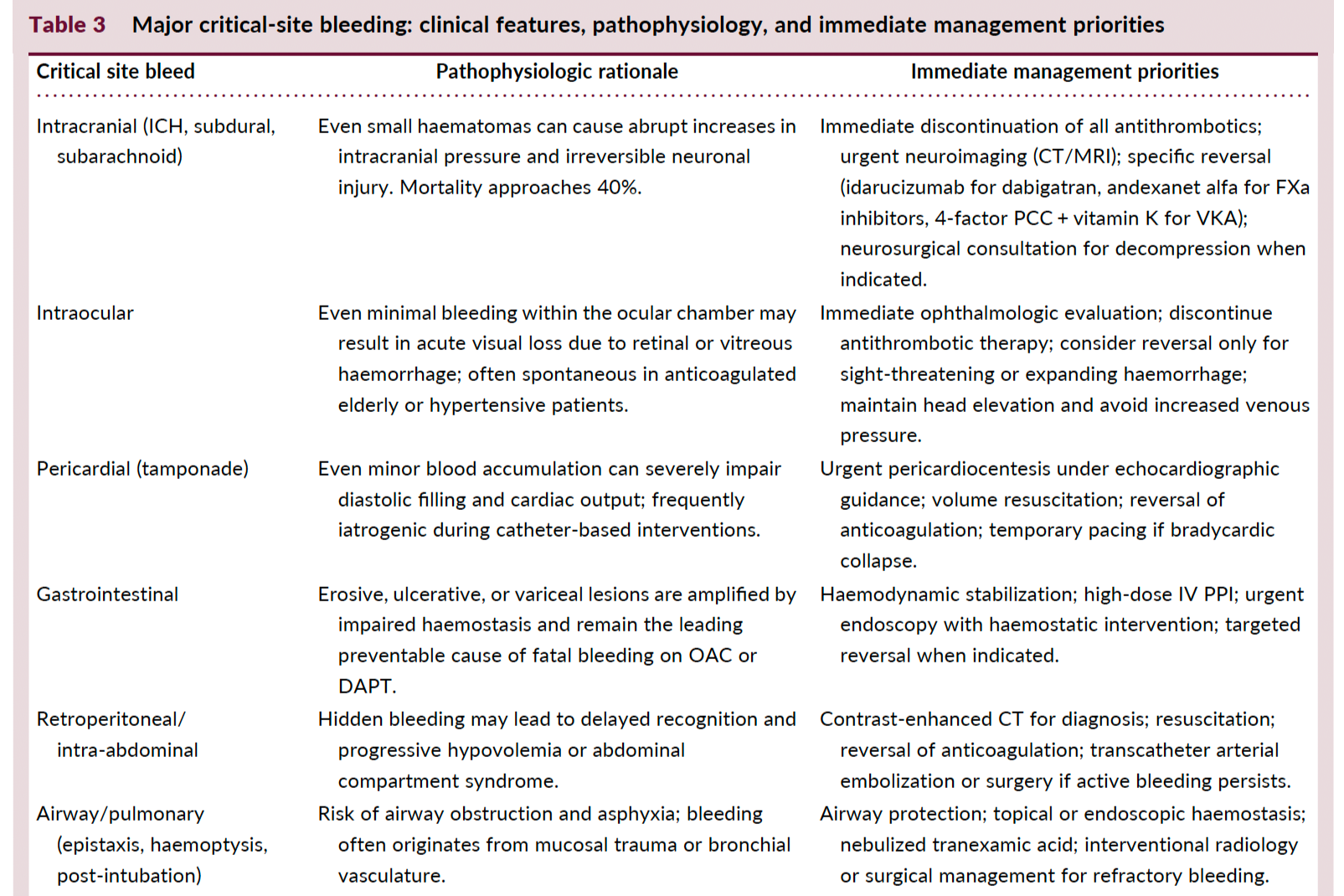
Hemodynamic instability or involvement of critical anatomical sites (e.g., intracranial, gastrointestinal) necessitates urgent stabilization, discontinuation of antithrombotics, targeted resuscitation, and, when indicated, anticoagulant reversal using drug-specific antidotes (idarucizumab for dabigatran, andexanet alfa or PCC for FXa inhibitors, vitamin K + PCC for VKAs).
Early intervention with multidisciplinary involvement enhances outcomes. Restarting OAC after major bleeding should be prioritized once hemostasis and source control are achieved, balancing the patient-specific thrombotic versus bleeding risk, and considering dose reduction or agent change where appropriate.
Minor bleeding is common but rarely requires hospitalization or cessation of therapy. Management is primarily supportive, focusing on local measures, correction of reversible risk factors, and avoiding unnecessary OAC interruption.
Admission heart rate and in-hospital mortality in acute myocardial infarction: a contemporary analysis of the MIMIC-III cohort
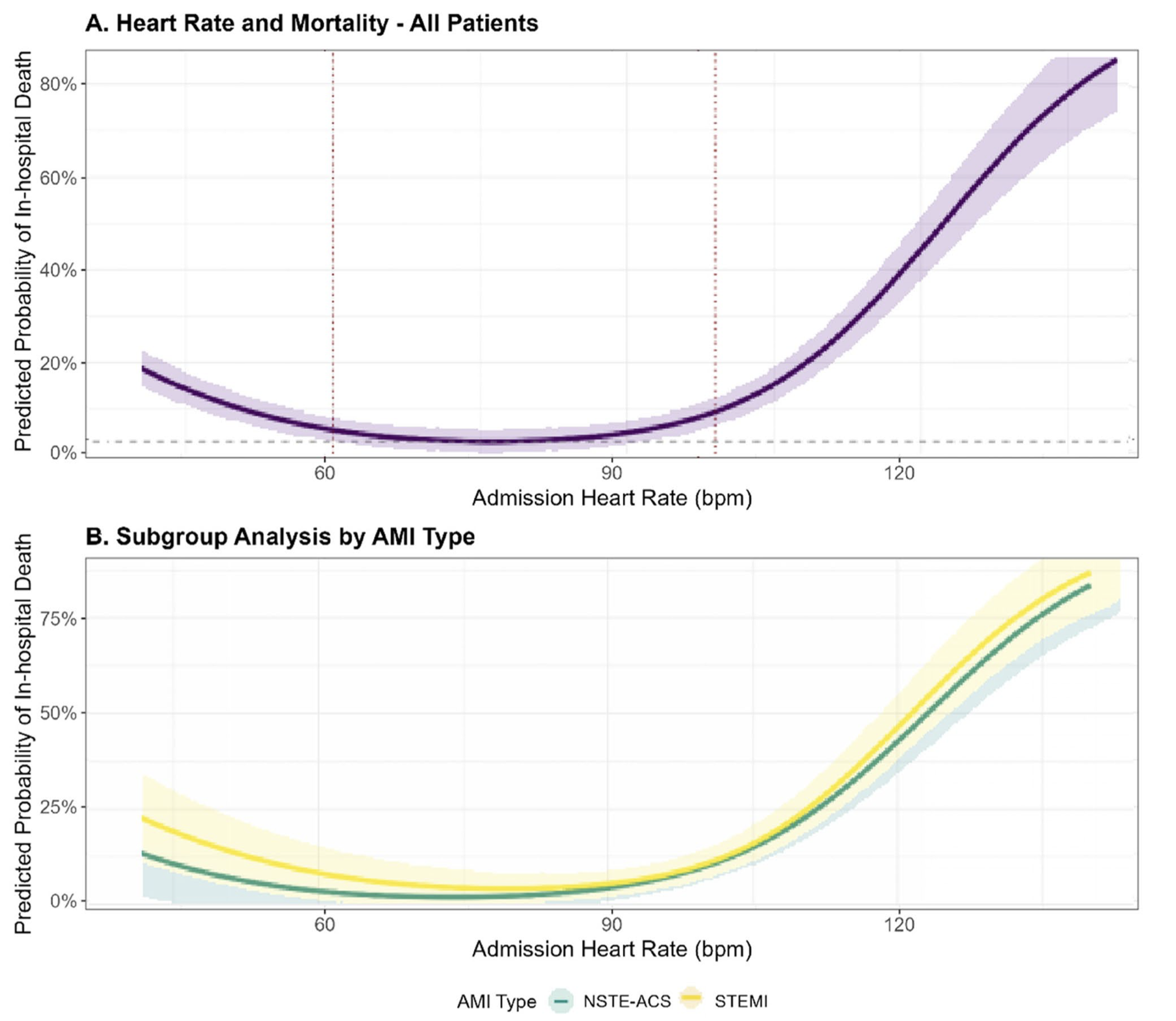
Admission heart rate (HR) in patients with acute myocardial infarction (AMI) exhibits a U-shaped association with in-hospital mortality, with both bradycardia (<60 bpm) and tachycardia (≥100 bpm) conferring significantly increased risk compared to the reference range (60–99 bpm).
After multivariable adjustment—including for age, sex, Killip class, systolic blood pressure, reperfusion therapy, comorbidities, and initial laboratory values—HR <60 bpm was associated with a 58% higher odds (aOR 1.58, 95% CI 1.02–2.45) and HR ≥100 bpm with a 145% higher odds (aOR 2.45, 95% CI 1.56–3.85) of in-hospital death.
The U-shaped HR–mortality relationship remained robust even after sensitivity analyses accounting for early mortality (<24 h).
This relationship is more pronounced in STEMI patients than in those with NSTE-ACS, with the steepest rise in mortality observed in STEMI patients presenting with tachycardia, and a somewhat greater impact of bradycardia in NSTE-ACS.
The optimal HR nadir for lowest in-hospital mortality differed by AMI subtype (≈78 bpm in STEMI and ≈72 bpm in NSTE-ACS), indicating a need for subtype-specific monitoring and intervention thresholds.
No significant effect modification by age, sex, hypertension, or early β-blocker use was observed, suggesting that the prognostic value of admission HR is consistent across these subpopulations.
Admission HR reflects integrated physiological responses, including autonomic tone, hemodynamic stress, and underlying conduction system disturbances, and thus serves as a rapid and practical risk stratification tool at the bedside.
Clinical implication: Patients presenting with admission HR outside the 60–99 bpm range MAY warrant prompt hemodynamic stabilization and closer monitoring, and prospective studies are needed to determine whether targeted HR normalization improves short-term outcomes in AMI.